Gynaecology
exp date isn't null, but text field is
ABNORMAL UTERINE BLEEDING
CLINICAL DESCRIPTION
Bleeding which deviates from normal menstrual pattern: internal, duration and amount. It may be acute or chronic.
Note: Episode of heavy bleeding requiring immediate intervention.
CLINICAL FEATURES
SIGNS AND SYMPTOMS
- Prolonged heavy cyclical bleeding, intermenstrual bleeding, cyclical bleeding
- If prolonged or heavy bleeding, may have tachycardia, palpitations, pallor, dizziness and general malaise.
INVESTIGATION
- Investigate for PALM-COEIN (Polyps, adenomyosis, leiomyomas, malignancy, coagulopathy, ovulatory dysfunction, endometrial causes, iatrogenic causes, none classified causes)
- Pregnancy test, clotting test
TREATMENT
- Stabilize (resuscitate) and then definitive management of cause.
- To reduce/stop bleeding
- Give high dose Ibuprofen 800mg 8 hourly for 5 days
- Give Tranaxemic Acid 1g 8 hourly po for up to 5 days
- Combined oral contraceptive 2 tabs daily for 10 days then 1 daily 2-6 cycles unless contraindicated. (For women over 40 years discuss with senior clinician before giving COC)
- Give Ferrous Sulphate 200mg daily for 2-4 weeks or until Hb is normal.
- Refer if persistent
- Adolescents, usually physiological, pathology rare
- Exclude pregnancy and its complications and manage conservatively
- If bleeding is heavy manage as above
- Women of childbearing age;
- Strongly suspect complications of pregnancy including ectopic pregnancy. Other causes; use of hormonal contraceptives, DUB, IUCD, fibroids, choriocarcinoma, cervical cancer
- Speculum examination mandatory to rule out local causes
Where no organic cause found
- Give Cyclic Progesterone 5-10mg 12 hourly for 14 days on second part of the cycle; alternatively, oral COC 1 od 3-6 cycles
- If no improvement refer to specialist
Post-menopausal women
- Important causes are endometrial cancer, cervical cancers, cervical polyps, atrophic vaginitis
- Always need investigation therefore refer early
AT THE HOSPITAL
- Speculum examination mandatory
- USS for masses and endometrial thickness. If >4mm, do obtain endometrial sample for histology.
ABORTION AND ITS COMPLICATIONS
CLINICAL DESCRIPTION
Loss of pregnancy before viability (gestational age less than 228 weeks or fetal weight less than 500g)
CLINICAL FEATURES
- Threatening: LAP, PV bleeding, no POC passed cervical os closed
- Inevitable: LAP, PV bleeding, no POC passed, cervical os open
- Complete: LAP, pv bleeding, POCs passed, os closed.
- Incomplete: : LAP, pv bleeding, some POCs passed, os open.
- Missed: Incidental finding of empty gestation sac or absent fetal cardiac activity on USS with no symptoms.
- Septic: Incomplete with features of sepsis and foul smelling POCS or discharge.
MANAGEMENT: OPTIONAL
Complications
Post abortal haemorrhage
- Resuscitate and stabilize the patient
- Carry out vaginal examination
- Remove products of conception and/or foreign bodies
- Give Oxytocin 10 units IM
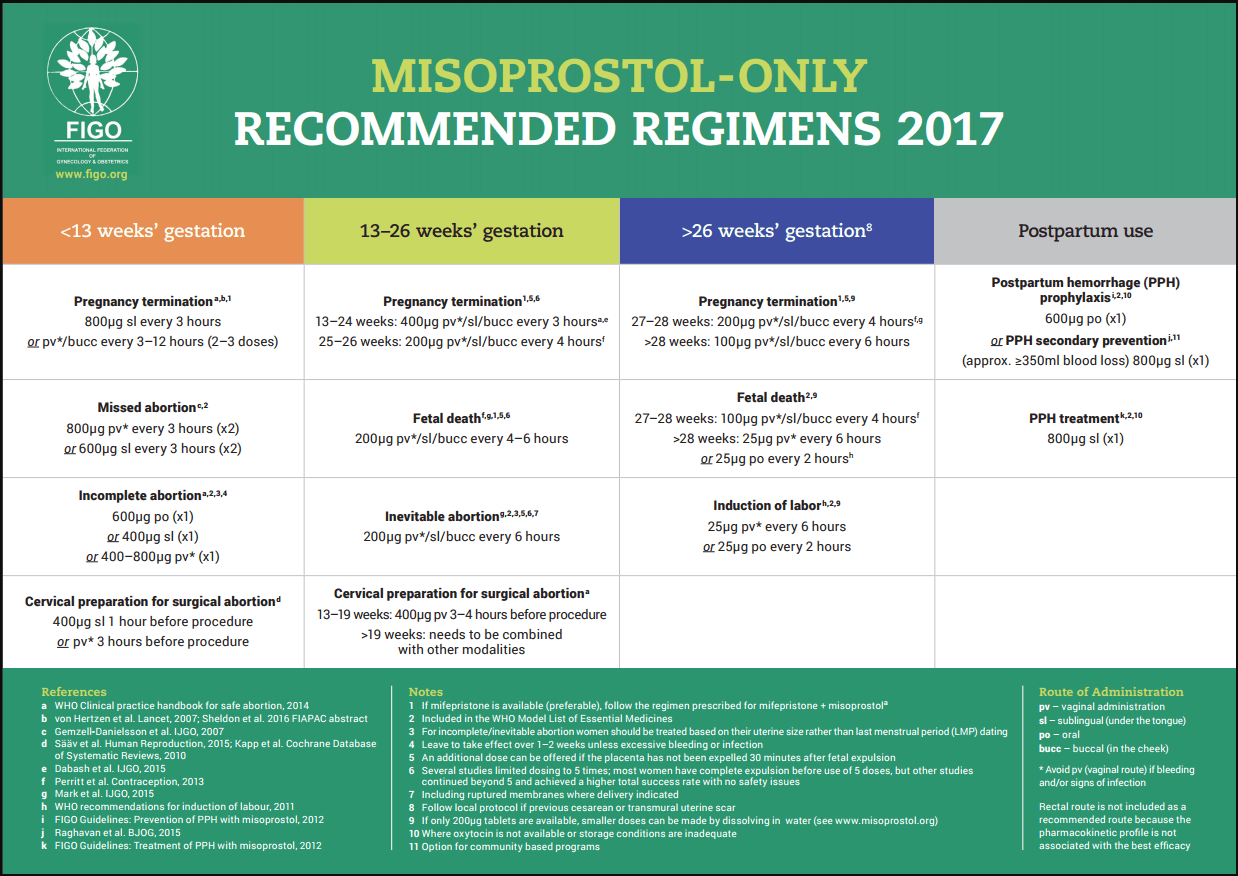
- Give Misoprostol 600mcg PO or 400mcg sublingually
- Comprehensive post abortal management plan
- Counselling for contraception, HTC, future fertility plans/pregnancy care
- Cervical cancer screening
- STI/HIV prevention and treatment
Missed miscarriage:
- Accelerate expulsion of the fetus with 200mg Mifepristone as a single dose followed by 800mg Misoprostol 48 hours later in first trimester (if mifepristone is not available, use misoprostol alone)
- REFER TO FIGO TABLE FOR A DOSES OF MISOPROSTOL

Inevitable
- Oxytocin 10 IU in 1l in the second trimester or await spontaneous expulsion.
Incomplete:
- MVA in the first trimester. Uterine evacuation for second trimester. For all cases of evacuation or MVA give prophylactic antibiotics prior to surgery: Give single STAT dose Doxycycline 400mg PO and Metronidazole 400mg PO
Complete
- Give single STAT dose Doxycycline 400mg PO and Metronidazole 400mg PO
- If patient is able to take PO medication, then provide full course of antibiotics.
- give Doxycycline 100mg 12 hourly for 7 days and Metronidazole 400mg 8 hourly for 7 days IV antibiotics
- If patient is septic
- Give Ceftriaxone 2g iv daily and Metronidazole 400 mg 8 hourly
- OR Ampicillin 1g 6 hourly/ Benzyl penicillin 2 MU IV 6 hourly, Gentamycin 240mg daily, Metronidazole 500mg 8 hourly IV fluids: N/S or RL
- MVA in the first trimester and blunt curettage in the second trimester
ECTOPIC PREGNANCY
CLINICAL DESCRIPTION
Pregnancy outside the uterine cavity. The fallopian tube is the common site for ectopic pregnancy.
CLINICAL FEATURES
SIGNS AND SYMPTOMS
- Often presents as ruptured
- Signs of hemorrhagic shock (low BP, high PR, confusion)
- Abdominal distension/tenderness
- Pain / tenderness in the iliac fossae
- PT positive
- USS: empty uterus
- Complex mass in the adnexa
- Free fluid in the abdomen/POD
INVESTIGATION
- Urine pregnancy test
- Ultrasound, FBC, Blood grouping save / crossmatch
TREATMENT
NON-PHARMACOLOGICAL
- Management: ABCDE approach
- Explain diagnosis and management to the patient
- If at the health Centre, refer immediately to the hospital after the above and communicate to the referral Centre
PHARMACOLOGICAL
- Insert 2 large bore IV cannula, take FBC and group and cross match samples, start Ringer’s Lactate or normal saline, catheterise
At Hospital:
- If first presentation is at the hospital, manage patient as above plus
- FBC, group and cross match
- Laparotomy stat (salpingectomy). Do not wait for resuscitation
- Cover for chlamydia with Doxycycline 100mg 12 hourly for 7 days
- Explain diagnosis and management to the patient
VAGINAL CANDIDIASIS (MONILIASIS)
CLINICAL DESCRIPTION
Common, excessive overgrowth of yeast in the vagina. Infection occurs more frequently in patients taking antibiotics, pregnant women, HIV/AIDS patients and patients with diabetes.
CLINICAL FEATURES
SIGNS AND SYMPTOMS
- Intense vulvo-vaginal itchiness, vaginal and vulval inflammation / redness, thick white rubbery discharge, superficial pain during sexual intercourse or during urination.
INVESTIGATION
- High vaginal swab and wet mount microscopy if available.
TREATMENT
PHARMACOLOGICAL
Adults:
- Give Clotrimazole 500mg intravaginal as single dose or Clotrimazole 200mg intravaginal once daily for 3 days
OR:
- Give Miconazole 200mg intravaginal once daily for 3 days
OR
- Give Fluconazole 150mg orally as single dose (contra-indicated in pregnancy)
OR
- Give Nystatin Pessary 100,000 IU vaginally 12 hourly for 7 days
To avoid re-infecting her partner, the male partner should:
- Apply the same vaginal cream as the patient
Recurrent vulvovaginal candidiasis should be referred to hospital
DYSMENORRHEA
CLINICAL DESCRIPTION
Lower abdominal pain just before or during menstruation.
CLINICAL FEATURES
SIGNS AND SYMPTOMS
- Lower abdominal pain just before or during menstruation
- Pain and cramping in the lower abdomen, lower back pain radiating down the legs.
INVESTIGATIONS
- USS for PID, endometriosis, fibroids, urine dipstick
TREATMENT
NON-PHARMACOLOGICAL
- Hot water bottle
PHARMACOLOGICAL
- Give Mefenamic Acid 500mg 8 hourly during menses for not more than 7 days
Alternatively
- Give Ibuprofen 400 mg 8 hourly {see section on analgesics}
- Diclofenac suppositories 100mg PRN
If no response:
- Give cyclical courses of Low Estrogen Combined Oral Contraceptive tablets once daily for 3 - 6 months
If there is still no improvement
- Refer to hospital
OBSTETRICAL FISTULA
CLINICAL DESCRIPTION
Abnormal opening or connection between the vagina and the bladder and the rectum.
Obstructed labour is the most common cause of urogenital fistula in Malawi. Other etiologies include pelvic surgery, radiation therapy and trauma or instrumental vaginal delivery.
CLINICAL FEATURES
SIGNS AND SYMPTOMS
- Draining urine or stools through the vagina
INVESTIGATIONS
- Speculum examination plus or minus dye test.
TREATMENT
NON-PHARMACOLOGICAL
Discourage early pregnancies.
- Encourage all pregnant women to attend antenatal care.
- Encourage health workers to use and interpret of partograph for laboring women
- Encourage all women to deliver at health facility
- Avoid delay in performing C/S
PHARMACOLOGICAL
- Catheterize patient with prolonged Labor for 5 days and give Amoxicillin 500mg 8 hourly and Metronidazole 400mg 8 hourly for 5 days.
At Health Centre
- Insert Foley’s catheter and refer all patients with draining urine and/or stools to the District Hospital
At District Hospital
- Reassess the patient to confirm the diagnosis with physical examination and dye test
- Insert urinary catheter and bring patient back for repair after 3 months.
Referral:
- Refer all complicated fistulae to the Central Hospital, such as: VVF of more than 2cm, rectal vaginal fistulae, ureteral vaginal and urethral vaginal fistulae