Abnormal Vaginal Discharge
exp date isn't null, but text field is
While a vaginal discharge is a notable clinical feature of a Sexually Transmitted Infection (STI), not all forms of vaginal discharge are abnormal or indicative of an STI. Vaginal discharge may be associated with normal physiological changes such as the menstrual cycle or pregnancy. Increased discharge may also occur with the presence or use of foreign substances such as the Intra Uterine Contraceptive Device (IUCD).
Careful history taking should reveal whether a vaginal discharge is abnormal and if it is associated with use of chemical substances e.g. topical self-medication, repeated douching with abrasive substances or indeed due to STI. Changes in the characteristics of a woman’s vaginal discharge either in colour, odour, amount and presence of additional symptoms and signs such as soreness and itchiness indicate a need for medical attention.
Abnormal vaginal discharge due to STIs may result in serious pelvic inflammation with sequelae such as ectopic pregnancy and infertility. Careful risk assessment is therefore required (see note below) of women presenting with a vaginal discharge in order to identify the possible causes and provide appropriate treatment regimens based on the most likely aetiology of the vaginal discharge. Factors that must also be considered when selecting treatment for patients include pregnancy status and patient discomfort.
Additionally, the syndromic approach must be used to assess the patient, identify risk factors and treat the likely cause of infection.
Cause
- STI-related
- Neisseria gonorrhoea
- Chlamydia trachomatis
- Trichomonas vaginalis (green or yellow, smelly, bubbly or frothy discharge associated with itching)
- Herpes simplex virus (following extensive first episode of infection)
- Non STI-related
- Candidiasis (white, lumpy or thick discharge associated with itching)
- Bacterial vaginosis (grey or white, fishy smelling discharge, especially after sexual intercourse)
- Gardnerella vaginalis
- Foreign bodies
- Herbal preparations
Symptoms
- Abnormal vaginal discharge - change in colour, odour, consistency or amount
- Vulval itching
- Vulval swelling
- Pain on urination
- Lower abdominal or back pain
Signs
- Abnormal vaginal discharge
- Vulval swelling
- Vulval erythema
- Lower abdominal tenderness
- Cervical excitation tenderness
- Cervical mucopus or erosions (on speculum examination)
Investigations
- High vaginal swab for microscopy, culture and sensitivity (if available)
TreatmentTreatment Objectives
- To identify and treat non-STI vaginitis
- To assess STI risk and treat STI-related infections appropriately
- To prevent complications and sequelae
- To treat both partners simultaneously as much as possible
Non-pharmacological treatment
- Promote good peri-anal and genital hygiene
- Encourage use of loose cotton underwear
- Dry underwear out in the sun
- Keep underwear dry
- Avoid douching with herbal or chemical preparations
- Avoid use of medicated soaps
Pharmacological Treatments
Risk Assessment:
- Parameters used in the risk assessment for cervicitis are:
- Patient’s partner is symptomatic (i.e. partner has a urethral discharge)
- Patient is less than 21 years old
- Patient is single
- Patient has more than one sexual partner
- Patient has had a new sexual partner in the last 3 months
The risk assessment is said to be positive and treatment for cervicitis is recommended if:
The answer to (i) is yes or
The answer to any 2 of items (ii) - (v) is yes.
If a woman has a vaginal discharge with no positive risk factor, treat for vaginitis alone.
If she has a vaginal discharge, and a positive risk factor, treat for both vaginitis
Treatment for Vaginitis due to trichomoniasis and bacterial vaginosis
Evidence Rating: [B]
- Metronidazole, oral, 400 mg 8 hourly for 5 days (contraindicated during the 1st trimester of pregnancy)
Or
- Metronidazole, oral, 2 g stat. (contraindicated during the 1st trimester of pregnancy)
Or
- Secnidazole, oral, 2 g stat. (contraindicated during the 1st trimester of pregnancy)
Treatment for Vaginitis due to trichomoniasis and bacterial vaginosis for pregnant women in the 1st trimester
- Clindamycin cream, 2%, vaginal, One applicator full at bedtime for 7 days
Treatment for Vaginitis due to Candidiasis
- Fluconazole, oral,
Uncomplicated: 150 mg stat. as a single dose
Complicated: 150 mg 72 hourly for 3 doses
Recurrent: 150 mg daily for 10 to 14 days followed by 150 mg once weekly for 6 months
Or
- Clotrimazole, vaginal tablets, 200 mg inserted into vagina at night for 3 days
Or
- Miconazole vaginal tablets, 200 mg inserted into vagina at night for 3 days
And
- Clotrimazole cream, vaginal, 1% or 2%, Apply twice daily for 3 to 7 days (for vulval irritation)
Treatment for Cervicitis due to gonorrhoea
1st Line Treatment
Evidence Rating: [B]
- Cefixime, oral, 400 mg stat.
And
- Azithromycin, oral, 1 g stat.
2nd Line Treatment
Evidence Rating: [B]
- Ceftriaxone, IM, 250 mg stat.
And
- Azithromycin, oral, 1 g stat.
Treatment for Cervicitis due to Chlamydia
1st Line Treatment
Evidence Rating: [A]
- Doxycycline, oral, 100 mg 12 hourly for 7 days (avoid in pregnant and nursing mothers)
Or
- Erythromycin, oral, 500 mg 6 hourly for 7 days
Or
- Azithromycin, oral, 1 g stat. (recommended in pregnancy)
Referral Criteria
Refer all cases of recurrent vaginal discharge and/or treatment failures to a health facility where speculum examination can be carried out and microbiological culture and antimicrobial sensitivity tests can be done on the vaginal discharge.
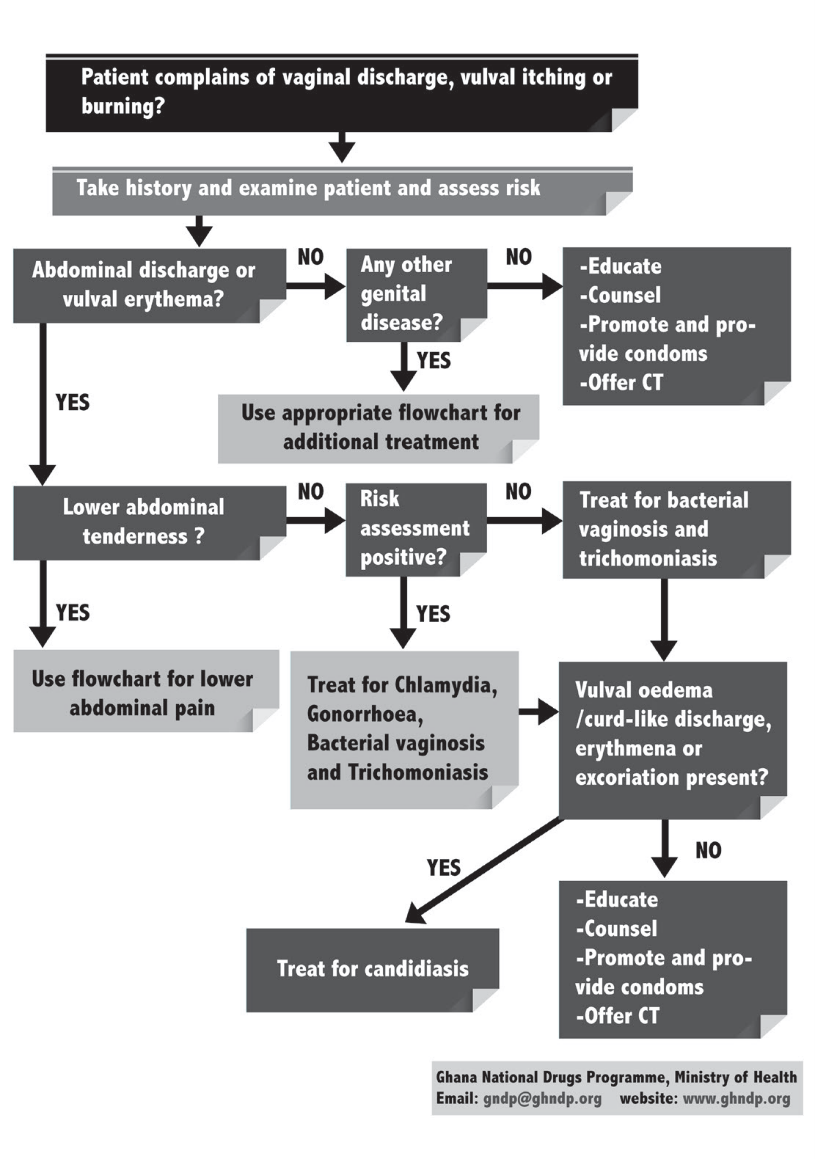
Flowchart: Abnormal Vaginal Discharge (Without Speculum)
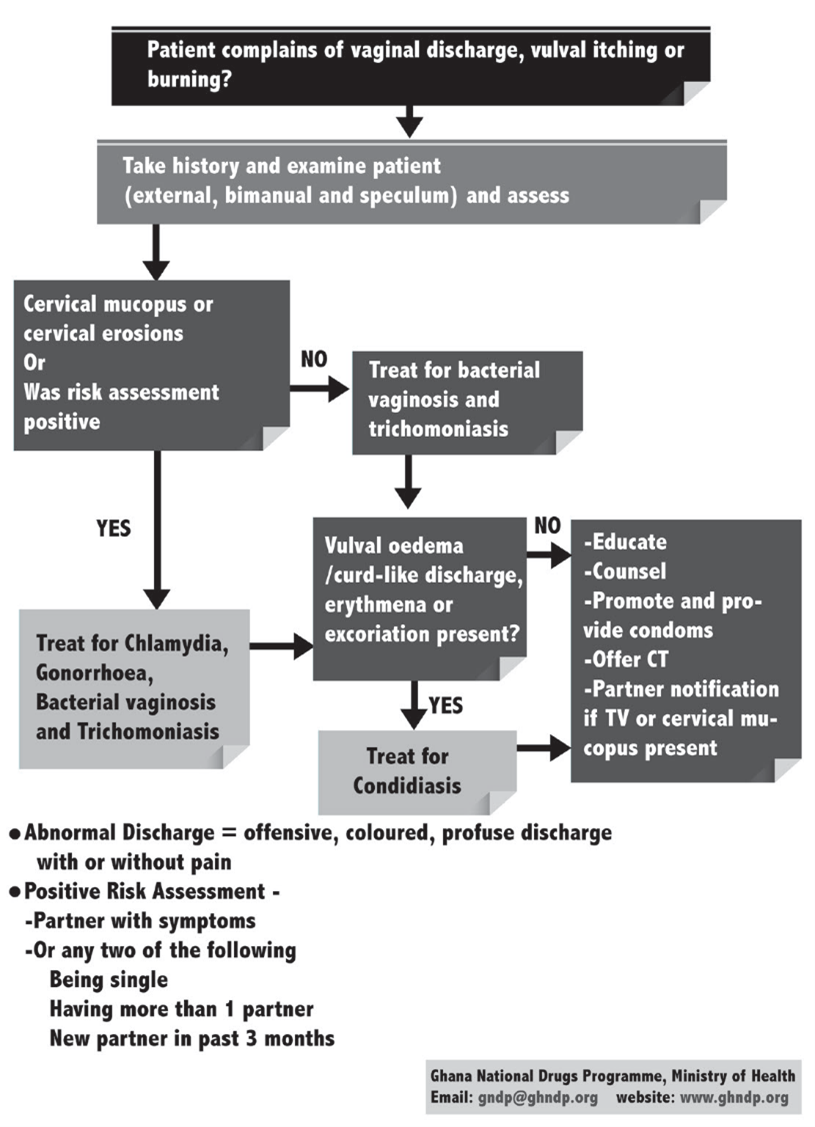
Flowchart: Vaginal Discharge with Speculum And Bimanual Examination