4.3 Hyperosmolar hyperglycemic state (HHS)
exp date isn't null, but text field is
HHS is a combination of severe degree of hyperglycemia, dehydration and hyperosmolality without significant ketonuria, usually seen as complication of elderly T2DM persons. Here, residual insulin reserve prevents ketosis.
4.3.1 Precipitating factors
Similar as DKA; also there may be:
- Compromised fluid intake
- Drugs e.g. glucocorticoids, diuretics etc.
4.3.2 Clinical features
- Develops slowly (days to weeks)
- Symptoms of uncontrolled diabetes precede
- Dehydration is profound
- Impaired consciousness
Table 4.2 Diagnostic criteria for DKA and HHS3
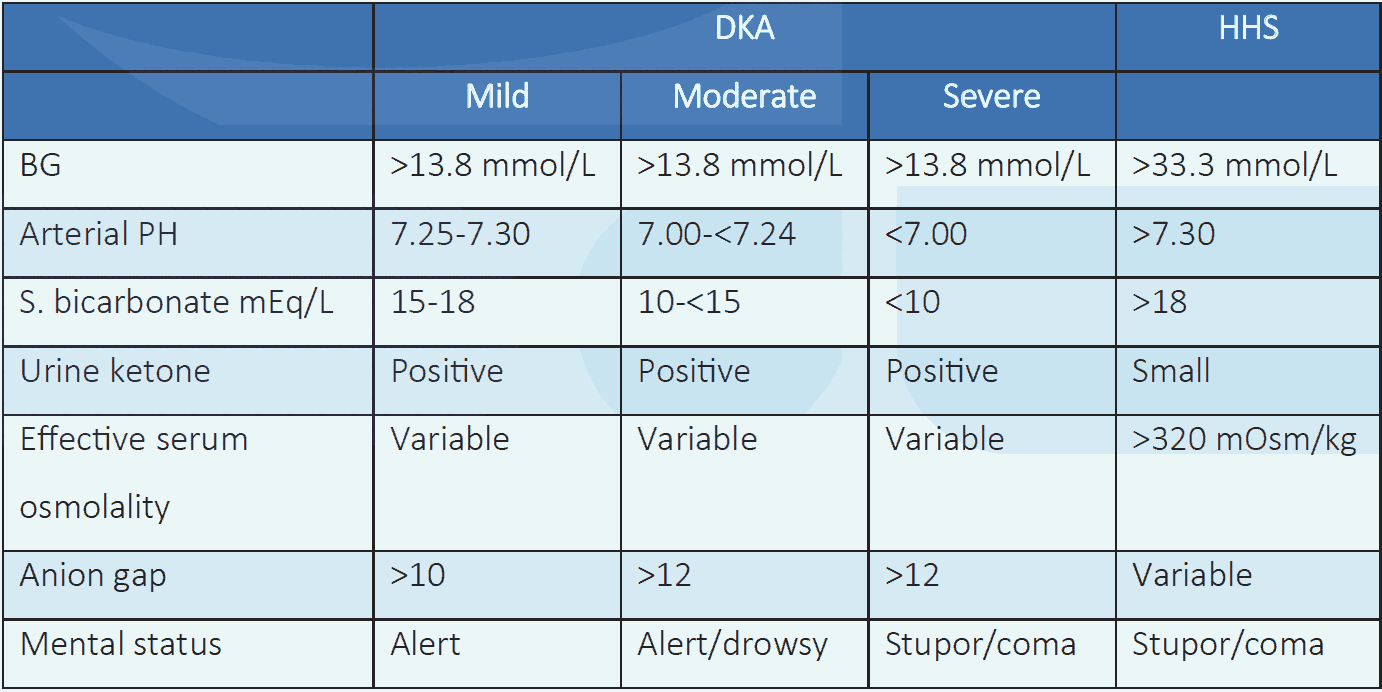
NB: Effective serum osmolality: 2[Measured Na+ (mEq/L)] + Glucose (mmol/L). Anion Gap: Na+ - [Cl- + HCO3- (mEq/L)].
4.3.3 Protocol for management of adult persons with DKA or HHS
Initial evaluation
- Immediate hospitalization
- Check blood glucose/capillary glucose, serum/urine ketones: to confirm hyperglycemia and ketonemia/ketonuria
- Test for blood pH, electrolytes, urea, creatinine, CBC
- Start IV fluid as per protocol
 NB: Corrected Na+ for hyperglycemia = Measured Na+ + [1.6 (glucose in mg/dL - 100)/100].
NB: Corrected Na+ for hyperglycemia = Measured Na+ + [1.6 (glucose in mg/dL - 100)/100].
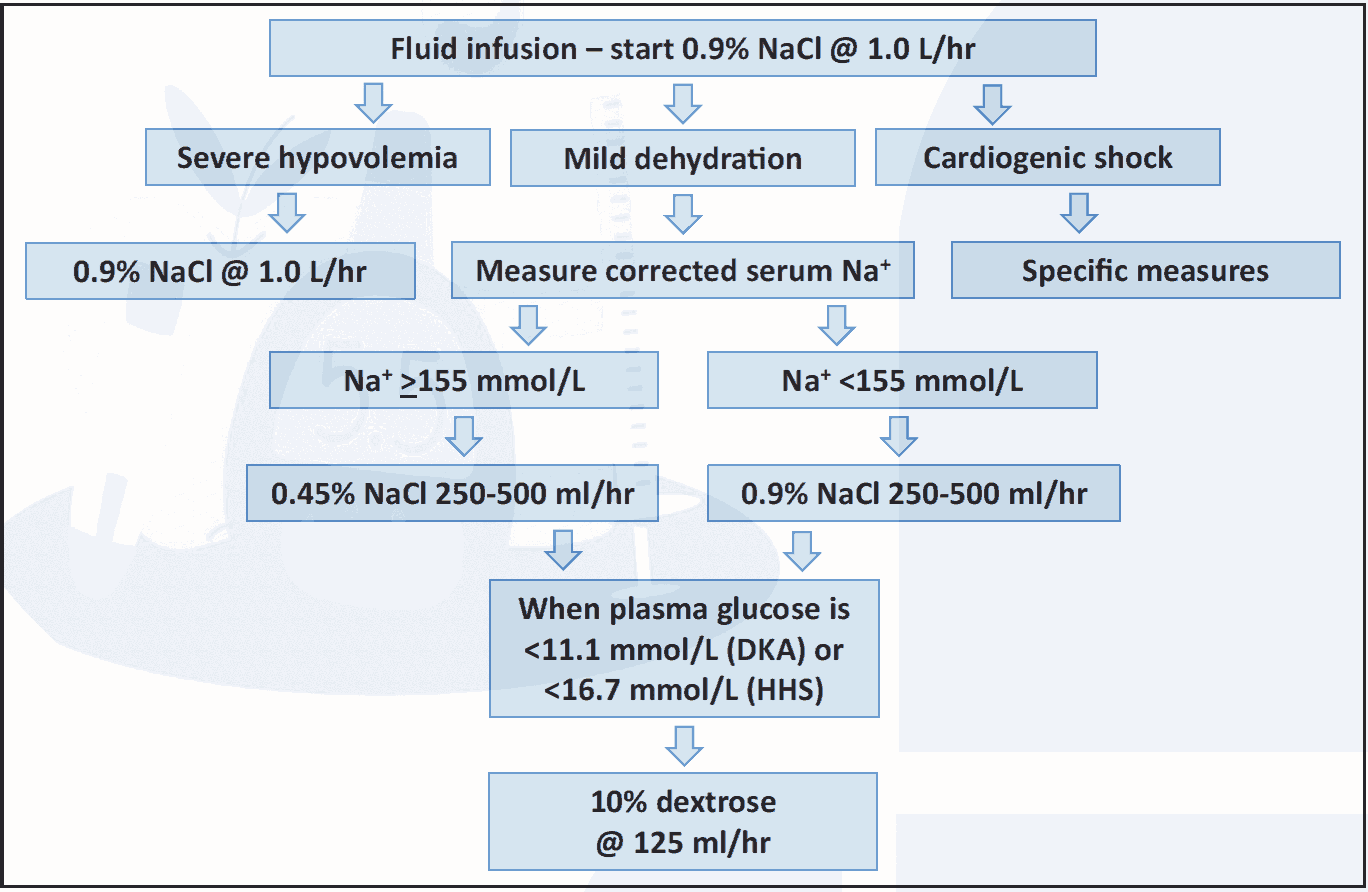
Figure 4.1 Fluid infusion protocol (DKA, HHS)3,4
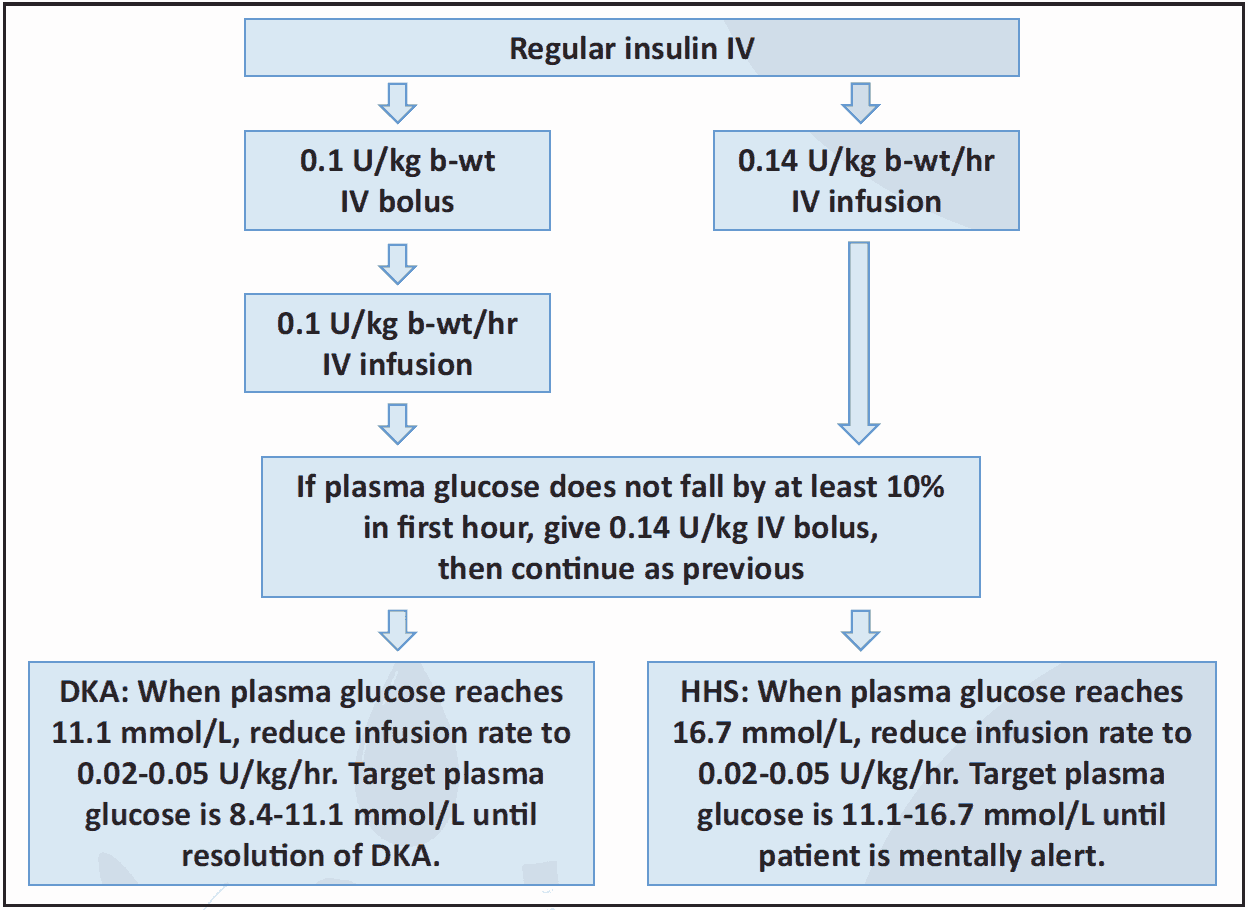 Figure 4.2 Insulin protocol (DKA, HHS)3,5
Figure 4.2 Insulin protocol (DKA, HHS)3,5
 Figure 4.3 Potassium infusion (DKA, HHS)3,4
Figure 4.3 Potassium infusion (DKA, HHS)3,4
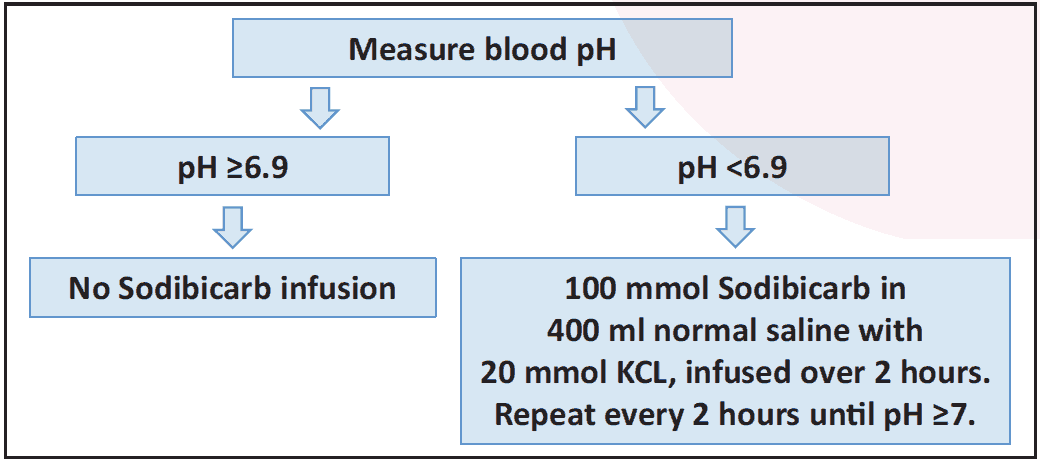 Figure 4.4 Bicarbonate infusion (DKA)3
Figure 4.4 Bicarbonate infusion (DKA)3
4.3.4 Other evaluations
- Blood glucose should be checked hourly initially.
- Blood pH, electrolytes, urea, creatinine should be rechecked frequently as required.
- After resolution of DKA/HHS and person is able to eat, SC insulin should be initiated. SC insulin should be started at least 1-2 hour before stopping intravenous insulin.
- During transition to SC insulin, multiply last 6 hours’ insulin dose by 4 to get 24 hours’ dose (TDD); from this initiate split-mixed or basal-bolus insulin regimen.
- Precipitating cause should be addressed.
4.3.5 Criteria for improvement of DKA/HHS3
- No dehydration
- No vomiting; able to take food
- Person is well oriented and hemodynamically stable
- No ketone in urine and anion gap normal (in DKA)
- Effective serum osmolality <315 mOsmol/kg (in HHS)
4.3.6 Complications of DKA/HHS2
- Cerebral oedema
- Circulatory failure
- Thromboembolism
- DIC