4.1 Hypoglycemia
exp date isn't null, but text field is
It is defined biochemically with blood glucose level below 3.9 mmol/L (70 mg/dL) with clinical features of autonomic over activity and neuroglycopenia.
Some people with DM, especially those with persistent high blood glucose, may develop clinical features (particularly autonomic) of hypoglycemia at a higher blood glucose level. Hypoglycemia is more common in T1DM than in T2DM.
4.1.1 Levels of hypoglycemia1
Level 1: blood glucose <3.9-3.0 mmol/L
Level 2: blood glucose <3.0 mmol/L
Level 3: a severe event characterized by altered mental and/or physical status requiring assistance.
4.1.2 Causes of hypoglycemia
- Taking excess dose of insulin
- Excess intake of antidiabetic medications, specially insulin secretagogues
- Delay, omission or undue reduction of a meal
- Unusual exercise
- Severe renal or hepatic impairment
- Over intake of alcohol
4.1.3 Consequences of hypoglycemia2
Recurrent hypoglycemia may cause behavioral change and cognitive impairment. Increased incidence of life-threatening cardiovascular events due to severe hypoglycemia.
4.1.4 Hypoglycemia unawareness and nocturnal hypoglycemia
Occurs in individuals with long standing T1DM, autonomic neuropathy, medications (like nonselective beta-blockers), or very tight glycemic control. Frequent blood glucose should be monitored to prevent hypoglycemia.
Nocturnal hypoglycemia occurs any time during night, usually between 2 and 4 am.
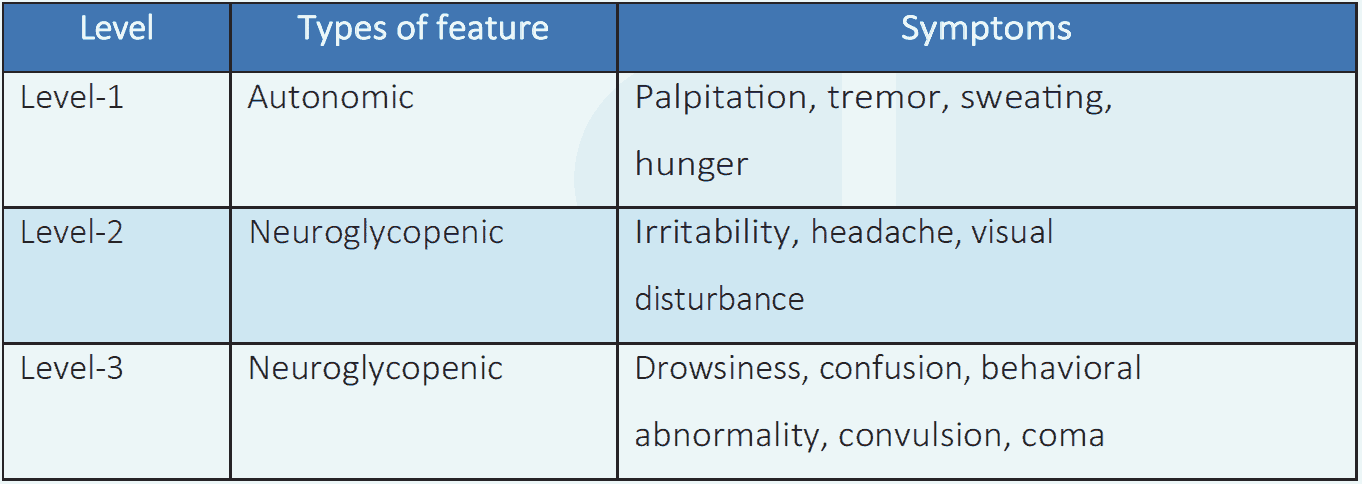
Table 4.1 Clinical features of hypoglycemia1
4.1.5 Treatment of hypoglycemia1,2
Level 1 and 2 hypoglycemia:
- Treated by the person him/herself or by a family member.
- It is usually relieved by 15 gm glucose or equivalent food, e.g. a glass of soft drink or fruit juice or snacks or meal (if it is due). These measures are usually adequate to raise blood glucose to reasonably safe limit (5.5 mmol/L).
- The food/drink is repeated every 15 minutes, and blood glucose should be checked every 15 minutes until the person is stable.
- Modification in ongoing treatment should be considered. Not to omit insulin/OAD altogether; dose may be reduced according to the condition.
- Glucagon 1 mg intramuscularly or subcutaneously can be given in those at increased risk of level 2 hypoglycemia if it is available.
Level 3 hypoglycemia
- 100 ml of 25% dextrose is given intravenously under medical supervision.
- If hypoglycemia is due to longer acting antidiabetic medications then 10% dextrose infusion should be started and may need to be continued for some time to prevent recurrent hypoglycemia.
- Ongoing activity of the antidiabetic medication may lead to recurrence of hypoglycemia. Hence, food ingestion is to be ensured after initial recovery.
- If recovery does not occur, addressing additional causes, modification in treatment and keeping the person under supervision in hospital may be required.
- Glucagon 1 mg intramuscularly or subcutaneously can be given if it is available.
Hospitalization criteria
- Level 3 hypoglycemia
- Recurrent hypoglycemia
- Hypoglycemia in people on long acting antidiabetic agents
Nocturnal hypoglycemia
- Reduction of evening dose of insulin
- Changing time of evening insulin dose with dinner time
- Taking bed time snacks may be considered
- These adjustments are made in conjunction with blood glucose monitoring
4.1.6 Prevention of ‘hypo’
- Frequent monitoring of blood glucose
- Proper meal timing and amount
- Avoid unaccustomed exercise
- Setting higher target for some people, e.g. older people, children, hypoglycemia unawareness